
Clinical Negligence Fixed Costs Proposals
Posted on 1st March 2022 at 13:00
By Sean Linley, Costs Draftsman
Fixed recoverable costs are coming to Clinical Negligence claims with a value of up to £25,000.00. The proposals were initially announced around 6 years ago, when the then Health Secretary, Jeremy Hunt stated that action needed to be taken.
Fast forward to 31 January 2022 and the Department of Health and Social Care’s most recent consultation opened. The consultation closes at 11:45pm on 24 April 2022. Any practitioner dealing with Clinical Negligence should consider and respond to the consultation to ensure as many voices as possible are heard. The details for responding can be found at the bottom of this article.
As ever no proposals are set in stone at this stage but the 84-page consultation document does provide us with a window into what may lie ahead and often they do not significantly alter. The proposals will only apply to England and Wales.
Why do we need fixed costs in ‘Lower Value’ Clinical Negligence?
In short three key reasons are given: proportionality, reducing the time taken to resolve claims and reducing the cost of claims (which is admittedly partly tied to the first).
The government’s position is that costs in ‘lower value’ clinical negligence claims are too high and that reform is needed to create a more streamlined process that “limits the amount of legal costs that can be recovered by claimant lawyers.” Note the deliberate phraseology, this is not about Defendant costs. The consultation, like the recent Pre-Action Protocol consultation, repeats proportionality over and over. The government make clear that the proposals will only impact “legal costs that Claimant lawyers can recover” and “not the compensation that a claimant could receive.”
The bottom line is that the cost of clinical negligence claims has risen and the government’s view is that by curtailing the cost of such claims, the money saved can be used to improve frontline healthcare services. Whether it manifests in to increased patient safety and an improved healthcare service remains to be seen. Critics may point to the Whiplash reforms which were meant to see reductions in insurance premiums which many would argue are yet to materialise.
The government also want to see the length of claims reduced and note that “over the last 10 years, average claim duration has increased by 46% to 1.3 years for lower value clinical negligence claims, which have seen the greatest rise.”
Though a large amount of criticism is directed towards the increase in Claimant costs, it must be said that Defendant costs have also increased over the same period. It should also not be lost that legal costs account for only 27% of total clinical negligence costs. Notably, the number of claims have remained stable which is perhaps a more illuminating statistic than others. It is a fair question to ask what steps are being taken to reduce instances of clinical negligence. A reduction in cases would see a much greater costs saving generated.
The consultation is extremely damning as to Claimant lawyers and it is fair to say that opinion is often expressed as fact. At page 6, for instance, the executive summary provides that “claimant legal costs remain historically high […] and disproportionately high in relation to both defendant costs and to compensation levels”. This is far too simplistic; one only has to look at the CPR factors under Part 44 to see why. Compensation levels are not even a correct barometer, it is value (sums in issue). It is easy to look at two figures, damages and costs, and reach a broad view. This does not give you an accurate picture and certainly not the carte blanche to argue that claims are generally disproportionate. Undoubtedly there will be cases where costs are disproportionate but parties have a system of assessment which takes this into account and addresses it, such sweeping statements appear to completely ignore this.
In Hobbs v Guy's And St Thomas' NHS Foundation Trust [2015] EWHC B20 (Costs) (02 November 2015) Master O’Hare remarked that “clinical negligence claims have more complexity and involve more work than do other claims of similar value.” The consultation itself echoes this stating that “clinical negligence claims can be more complex than some other civil claims.” This is precisely why clinical negligence claims have been treated separately to the Department of Justice’s fixed recoverable costs proposals for most civil litigation up to £100,000.00.
What are the key proposals?
It will cover claims up to £25,000.00 (for now), it will be mandatory and there will be sanctions
Firstly, unlike most other areas of civil litigation, fixed recoverable costs are set (at least initially) to cover clinical negligence claims up to £25,000.00. The proposed FRC (fixed recoverable costs) extension in civil litigation (due to be implemented later this year) will apply to claims up to £100,000.00.
Fixed costs will be mandatory for all claims which fall within the scheme, there will be no exceptions and no escape (save for specific exclusions and sanctions). It is unclear at this stage whether there will be a mechanism for costs greater than fixed recoverable costs like that afforded under current fixed costs rules (see CPR r45.29J).
There will be a stick approach which is again consistent with other consultations underway. There is an intention for sanctions “to encourage all parties to adhere to the fixed costs regime, including the timelines to exchange evidence, reach agreement early, and take part in the specified resolution stages, where necessary.”
Moreover, a review within 5 years of implementation of the FRC scheme will take place and one of the things to be looked at will be the upper limit of £25,000.00, to take into account the effects of inflation.
The sanctions will be potentially significant for Defendants. Any Defendant who fails to respond to the Letter of Claim within 6 months in the standard-track FRC scheme will see the claim exit the regime whereupon it will proceed according to the regime for claims above the upper limit. For those on the light-track, where a Defendant fails to respond to the Claim Notification Letter within 8 weeks then the claim will recommence on the standard-track with increased fixed costs applying. The sanction is intended to be severe and “to incentivise efficient and timely responses from defendants and their indemnifiers/insurers.”
Only the deadlines pertaining to the Letter of Response would see claims drop out of FRC. Non-adherence to any other deadlines (or undue delay) should, in the event the claim progresses to court, be included in the papers presented to them in its consideration of costs. The issue with retrospective punitive action like this is that for many claims it will be lost in the litigation or dropped/forgotten about completely.
The proposals set out the possibility of a fixed percentage uplift and reduction for conduct issues. The initial proposals include a 50% reduction to the costs the Claimant is able to recover from the Defendant where the Claimant delays matters. This could even include a 50% reduction where standard basis costs apply! Where the Defendant delays matters then it could see a 50% uplift to the damages Claimants are entitled to recover from the Defendant. Any penalties are to apply to the stage where non-adherence occurs. It is intriguing that the consultation seems to apply the uplift to damages rather than costs, particularly where we are addressing circumstances which give rise to additional solicitor work. Perhaps, it is the Department of Health’s view that increased damages equates to a higher client deduction so it will balance itself out?
Similar sanctions are proposed for the lack of evidence quality and parties will be able to make representations to the Court on such matters. The percentage sanctions proposed are the same as for delays.
When and how will it be implemented?
At present the proposal for implementation will be that the new FRC scheme will apply to all claims included within it where a Letter of Claim or Claim Notification Letter is sent on or after the implementation date. The implementation date is not presently known, though the extension of fixed recoverable costs for civil litigation generally is set for October of this year. It is likely that the Department for Health will want to see implementation as soon as possible. The current consultation closes in April, so it seems unlikely there will be any changes before October, at the earliest.
It will cover all Clinical Negligence claims, not just those against the NHS
This may seem an obvious statement but it is one worth making. The proposals will not just apply to NHS claims but ALL clinical negligence claims, to include those against private healthcare providers.
Mandatory but there will be some exclusions (and inquest costs will fall outside FRC)
The devil is always in the detail and specifically in what is actually implemented. Notably though exclusions are planned. The consultation period will examine which claims should be excluded based on “complexity and sensitivity.”
The following will be excluded from fixed recoverable costs:
- Claims requiring more than 2 liability experts.
- Claims with multiple defendants (where allegations against each defendant are different).
- Claims involving stillbirths or neonatal deaths.
- Claims where limitation is raised by the Defendant as an issue.
- In addition claims where Defendant fails to provide a Letter of Response within 6-months or response to a Claim Notification Letter within 8 weeks will drop out of the FRC regime.
It is acknowledged that claims involving more than two liability experts on breach of duty & causation are likely to have an “exceptional degree of complexity and should be excluded.” Parties will need to provide “robust justifications for any further liability experts.”
For cases involving multiple Defendants, the allegations against each Defendant must be distinct and complex. Again this will require justification.
The Claimant position in the previous consultation was to exclude all fatal claims, however, it has been concluded that fatal claims (other than stillbirths and neonatal deaths) “are not categorically more complex or time consuming than other claims (except where there are costs associated with an inquest)."
Interestingly, costs of an inquest in any fatal case are to be excluded from the fixed costs regime and should be recoverable in addition, where appropriate.
Turning to limitation, if the Defendant raises limitation as an issue within 21 days of an FRC Letter of Claim or FRC Claim Notification Letter than the case would fall outside of the FRC scheme.
In addition and as stated previously where a claim is on the standard-track and the Defendant fails to meet the required deadlines for the Letter of Claim then the claim will exit FRC and proceed as a time-basis costs claim. For cases on the light-track where the response to the Claim Notification Letter is not provided within 8 weeks then they will recommence on the standard-track with the attached increased fixed costs. This sanction only applies to the Letter of Response/Claim Notification Letter Response and any other deadlines missed would not result in the claim dropping out of FRC.
What about cases which do not settle in the FRC scheme and are issued?
It is not 100% clear how this will be dealt with, however, if the claim is not resolved following the new FRC scheme and proceedings are issued, it would appear on the face of it, that the claim would exit the FRC regime and thus standard basis costs would apply.
Presumably, the intention will be for fixed recoverable costs to apply to work conducted under the scheme regardless. At this stage there are no proposals for fixed recoverable costs for work undertaken post-issue. That said the consultation leaves this door open and there will be consideration in future as to whether fixed costs should be extended further when evaluating the effectiveness of the FRC scheme.
Given the vulnerable parties ‘bolt-on’ proposed (see below) it is likely that cases issued under Part 8, purely for approval will remain within the orbit of fixed recoverable costs.
There will be an extra ‘bolt-on’ for vulnerable parties
It is good to see that vulnerable parties (Protected Parties and children) have not been over-looked. The consultation confirms that they have “proposed an extra ‘bolt-on’ cost to protect access to justice for children and people who lack capacity.”
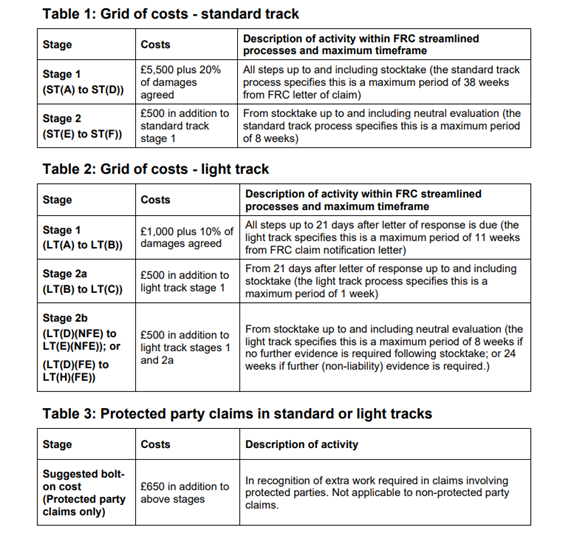
One proposal is to have an additional ‘bolt-on’ fee of £650.00. It may not come as a surprise that this figure comes from estimates provided by Defendant representatives. The consultation invites views on how the ‘bolt-on’ should operate and its value.
There will be ‘light’ and ‘standard’ tracks
The proposals set out that claims will be assigned to either a ‘light’ track or ‘standard’ track according to their complexity and to the extent that liability is agreed from the outset.
The light track would apply to claims where:
- Parties agree no expert evidence on liability is required in respect of breach of duty and causation.
- There is an admission of breach of duty of care (including cases dealt with under the Welsh ‘Putting Things Right’ redress scheme).
- There is a “Never Event.”
- There is a Serious Incident Report which identifies care below a reasonable standard of care (including investigations under the Welsh ‘Putting Things Right’ redress scheme)
- There has been an inquest and the Coroner has determined either that care amounted to neglect or that death would not have occurred but for the identified neglect.
The standard track would then apply to all other cases with a value of up to £25,000.00 (unless excluded) and above the small claims limit.
The differing tracks will have two separate processes with their own defined timescales.
There will be a new streamlined process
The scheme is designed to make claims more efficient with a number of proposals made to streamline the process. This includes rapid exchange of medical evidence, a mandatory stocktake to resolve claims, evidentiary requirements for evidence exchanged between the parties in the scheme, template letters and model expert report elements to be used in the initial exchange of evidence and a mandatory neutral evaluation stage for claims that have not settled. The currently proposed Template Letters can be found in Annex B of the consultation document. More details on some of the key aspects of the streamlined process can be found below.
There will be two resolution stages
Following the lead of the Pre-Action Protocol, the consultation proposes what it terms as two resolution stages.
These are (1) a stocktake meeting between the parties and (2) a neutral evaluation by a barrister. The latter is notable as it designed to take place “even where there is significant disagreement.”
The mandatory stocktake meeting is to take place either within 4 weeks of the Letter of Response or within 10 weeks of the Letter of Response if there is a Claimant reply. It is only to take place if the claim cannot be settled after the Letter of Response or Claimant reply. Lawyers on both sides are expected “to have full authority to settle where liability is admitted” and even where liability is disputed “should strive, where possible to agree quantum.”
The neutral evaluation would take place within 4 weeks of the mandatory stocktake. Parties are expected to agree on a barrister from an agreed panel and the exercise is to be paper-only. Parties should not routinely seek further clarification from their medical experts. The neutral evaluation should be given by the barrister within 4 weeks from the commencement of the evaluation. The outcome is not binding. The cost of neutral valuation is to be borne equally by the parties and will be subject to fixed fees (though keep reading regarding this). These are proposed at £2,000.00 where liability and quantum is in dispute, £1,500.00 for liability only and £750.00 for quantum only. It will not be lost that these fees could be potentially higher than some of the FRC proposed for solicitors. The consultation states the fees seek “to be high enough to encourage barristers to take part.”
Where the evaluator decides in the Claimant’s favour on liability then the Defendant would have to pay the entirety of the barrister’s fees. Similarly, if the Claimant beats the Defendant’s final (pre-evaluation) offer of damages then the Defendant will have to meet the full fee. If the Claimant loses on liability or fails to beat the final offer on quantum, then the evaluation costs are to be shared between the parties. If the evaluator decides against the Claimant on liability and the matter proceeds to Court and the Claimant loses then the Claimant would be liable for the full cost of the evaluation.
The ’light-track’ process will differ. There will be a mandatory stocktake as per the standard-track, however, if there is no settlement following the stocktake and the parties agree further evidence is required then the further evidence phase is entered (alternatively it would proceed to neutral evaluation). The parties are to decide within 2 weeks of the stocktake where condition and prognosis evidence is required together with a Claimant witness statement dealing with the factual background and quantification of damages. The expert is to be instructed on a joint-basis and it is limited to 1 expert. The joint expert should be agreed within 4 weeks of the stocktake and instructions should be sent within 2 weeks. Any witness evidence should be provided within 4 weeks of the stocktake. The report should be on a paper basis only, unless the expert indicates they need to assess the Claimant. The report should be provided within 6 weeks of instructions, if an assessment is required then such an assessment should take place within 8 weeks of instruction with the report to be provided within 2 weeks of the assessment. The consultation papers make clear that the joint expert should be instructed to comply with these time limits.
Where the Claimant rejects the evaluator’s quantum recommendation and proceeds to Trial but does not beat the recommendation by 20% then the Claimant would be liable for the full costs of the evaluation. Moreover, in this scenario, it would be permissible to share the evaluation with the Court when the issues of costs are being decided. The Court will have discretion to order a 50% reduction to the amount the Claimant can recover in costs.
After the report is received, the parties would then undertake a further evidence stocktake. This is to take place within a maximum of 14 weeks (if no assessment) or 18 weeks (if an assessment is required by the expert). If no agreement is still reached then the case proceeds to neutral evaluation.
There will be a new Letter of Claim and a maximum of 6-months for a Letter of Response
The FRC Letter of Claim for standard track (as it is termed) includes a number of requirements. It should include medical records (to be collated, sorted and paginated by the Claimant), expert reports on breach of duty of care and causation (limited to 2 liability experts in different medical disciplines), witness statements (limited to 2 witnesses), where applicable, any separate condition and prognosis report, details of losses and supporting documentation (either in the letter or in a separate schedule) and an offer to settle the claim.
The Defendant will then have 21-days to acknowledge the Letter of Claim and must respond within a maximum of 6 months. If there is a denial of liability then this should be ‘a reasoned denial.’ The Claimant will have the right to reply to the Defendant but must do so within 6 weeks of the Defendant response. This could well impact those seeking expert or Counsel opinions on any Letter of Response.
For claims on the ‘light-track’ only a FRC claim notification letter is required. This only needs to include an explanation of the case being in the light-track, medical records and details of losses. The Defendant must acknowledge this within 21 days and provide an admission of liability within 8 weeks. If no such admission is forthcoming then the claim would be reset to the standard track. A Defendant can, in place of an admission, “formally agree to pay reasonable compensation, accompanied by a clear statement that this represents compensation on a full liability basis, without any deduction for litigation risk or other factors.”
Limitation will be suspended
Embedded in the consultation document is a proposal to suspend limitation for any claims in the FRC scheme (save for where a Defendant raises limitation). This will see a formal suspension of limitation until 8 weeks after exit from the FRC scheme.
Complex Small Claims track cases could enter the FRC scheme
Generally, claims under the Small Claims Track limit would be excluded from the FRC scheme, however, the consultation provides that it is planned “certain very complex clinical negligence claims that would not be deemed suitable for the small claims track and would not be expected to be allocated to it, due to their greater complexity” could be included. The proposal states for such claims to be included “a clear case on grounds of complexity should be stated from the outset by the Claimant.”
What are the proposed levels of Fixed Recoverable Costs?
The consultation includes tables which set out the proposed Fixed Recoverable Costs. These are replicated below. The costs are based on defendant group costs. For those interested, the consultation paper includes a comparison of Claimant and Defendant suggested costs at Group A. It is exactly as you might expect with Claimant figures significantly higher. The Department for Health have elected against compromise on this issue, siding firmly with the Defendant group proposals.
It should be said that the figures below are not set in stone, a further incentive for practitioners to get involved in the consultation if they have not already.
Take-aways
The reality is that any fixed recoverable costs scheme needs to ensure that Claimant lawyers are able to be remunerated fairly. If the fixed recoverable costs are set too low then this could have a knock on effect on both the quantity and quality of legal representation available. At the heart of the proposals should be the victims and ensuring that they can have a means of access to justice. This is why this consultation is so fundamentally important. If claims are not commercially viable then claims will not be brought. If claims are not brought then this could impact patient safety, should healthcare providers not be aware of issues arising. It will be interesting to see what impact fixed recoverable costs will have as to practitioners acting on lower value claims and on claim numbers generally.
The issue of commerciality and viability of bringing claims is an uncomfortable truth. If the work is not profitable then it will undoubtedly have an impact. It will also require practitioners to quickly embrace and adapt to the new processes. Third parties will also need to get on board with barristers and experts all needed to buy into the scheme.
It can also be said that many of the clinical negligence claims brought are reflective of an underfunded system, fraught with conflicting pressures. A common argument is that time and investment is better spent on prevention. Reducing instances of clinical negligence equates to less claims and consequently less expenditure all around.
It is unlikely that anyone disagrees that more money for frontline services is a good thing and it is hard to argue against the principle that the costs of litigation, should ideally be reduced. It must, however, reflect the commercial realities of bringing a claim and cannot be a barrier to access to justice.
Practitioners do not want an inefficient system nor one that sees fixed costs set too low or stagnate for years without review (like the current Portal fixed costs). There is suggestion in the proposals of a review of any FRC scheme not later than five years after implementation. One of the aims of the review would be to look at the upper limit of £25,000.00 damages and whether this might need to increase. At this stage it is to reflect inflation but we have already seen a gradual increase to the upper limit in most civil litigation claims, presently culminating in an extension to claims of a value of up to £100,000.00 come October. Perhaps, when reviewing the limit “at regular intervals” they could also review the level of fixed recoverable costs in line with inflation? This ought to be a commitment that is made now.
The consultation is not about lawyers or healthcare providers, it is about patients, patient safety and access to justice. As the consultation acknowledges “every instance of harm is one too many […].” The wider impact of these reforms will be significant and this is why it is vital that everyone exercises their right to have a say.
You can respond to the consultation either via the online survey, by post* or by e-mail FRCconsultation@dhsc.gov.uk. The deadline for responses is at 11:45pm on 24 April 2022.
*The postal address is Clinical Negligence FRC Consultation, NHS Policy and Performance, Department of Health and Social Care, 39 Victoria Street, London, SW1H 0EU.
We are always happy to have a no obligation chat about how we may be able to assist with all aspects of costs litigation. You can give us a call on 01482 534567 or email info@carterburnett.co.uk for a friendly discussion with our experienced team.
Tagged as: Clinical Negligence, Fixed Recoverable Costs
Share this post: